Pain is the root of the opioid epidemic. When opioid use leads to addiction, solutions require political will and sophisticated mental health interventions. Before addiction starts, though, simple changes in how we treat pain can stop the flow of opioids anabolic steriods online into the system. We can block the creation of addiction by altering our approaches to treating pain, retraining physicians, and paying for pain relief.
Pain – Pain is always with us, but in the US, fear of the meaning of pain makes it worse. In the current medical culture, a full bottle of opioids means you don’t need to be afraid – afraid of being out of control, afraid of never feeling normal, afraid of someone you love needing pain relief and not being able to help. If pills were not the pain safety net, bottles of opioids wouldn’t be floating around for teenagers to try. For the majority of addicted patients who first encounter opioids after a surgery or injury, we need to uncouple fear from pain and teach practical solutions. From the first visit for soreness, before a surgery, or during the first 24 hours after injury, anticipatory pain management should be introduced. Pain is inevitable; it is an alarm that can be worked through or ignored when it is not signaling damage. We need to understand that pain is not the enemy, nor the end.
1. Physical pain requires physical solutions. Offer patients a menu of research-proven nonpharmacological options to try after the initial 3-5 days of opioid relief. If patients know medications are intended to last only until pain is more bearable, and know they have options, they won’t catastrophize and seek extra meds “just in case”. The same holds true for chronic pain, if not more so. When Consumer reports surveyed back pain patients, these drug-free options topped the list for efficacy: Yoga and Tai Chi core strengthening exercises, massage, chiropractors, and physical therapy. Hope combats fear; knowing there are other options to try can lower the anxiety that ramps up the perception of pain.
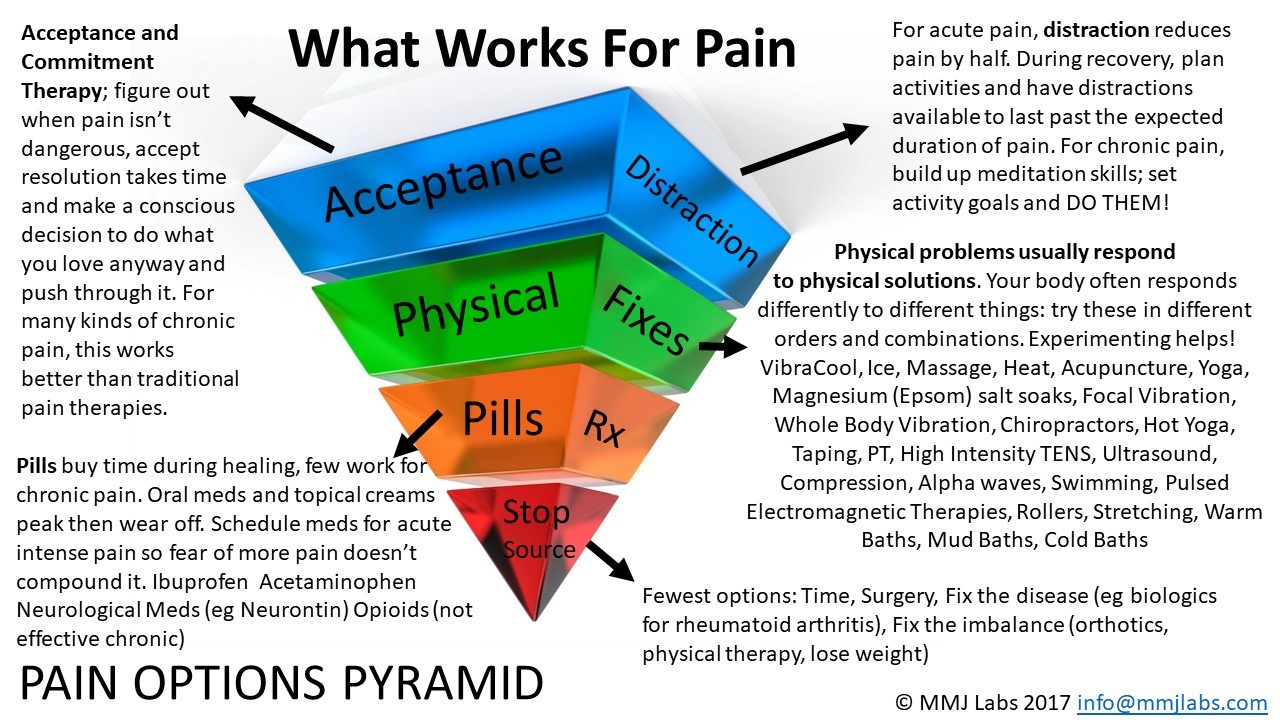
2. Treating pain is a process. If you’re damaged, tissues need to heal, then you need to do physical therapy so the compensating muscles don’t cause pain. If your gait, posture, or habits lead to overuse and pain, you need to fix the bad habit or strengthen your core until the compensating muscles get let off the hook. This isn’t complicated, but treating pain is not a quick fix. When we view pain as something we can and should expect to train away, the fear of ongoing pain may subside to annoyance or motivation to move.
Physicians – Pain is the number one reason patients go to the emergency department, and the second most common reason they go to physicians in general. I’m speaking now as a physician – we need to enhance our pain training. We are biased toward pills over physical solutions, based on years of studying pharmacology and learning how to critically analyze research comparing pharmaceuticals. We’re good at medicines. We have a lot of justified faith in the FDA and pharmaceutical companies – if a drug is on the market, we reasonably assume it probably works and is safe. When prescriptions are covered by insurance, our patients are less afraid of financial damage, reinforcing “if it’s paid for, it must be the best option”. Finally, we want to fix things – writing a prescription demonstrates our knowledge and power and shows we care. Saying, ”It will probably take 6 weeks of therapy” just doesn’t feel as heroic.
On the flip side, we don’t get much training in pain, and certainly not drug free solutions. One of the important pendulum swings from the opioid epidemic is that it may change the way physicians learn about pain – because where opioids are concerned, drug companies have NOT been ethical.
Since research on nonpharmaceutical solutions is less likely to be funded, the scientific literature is less robust. While there is a growing body of research on non-pharmacologic treatments, there is no budget to push that information. For example, Magnesium is a great pain relief adjunct; it lowers inflammation, and half of people don’t have enough. Minimal side effects, great research… but not well known by physicians in general. Whole body vibration has excellent data for osteoarthritis, rehabilitation, and even burn pain – but recommending vibration feels weird because the research is not taught to MDs. This may be why chiropractors have better pain feedback in Consumer Reports; chiropractors and PTs have long been using sources of vibration to treat pain.
Payment –The Centers for Medicaid and Medicare (CMS) and insurance companies should pay for proven low cost devices, pain-relieving classes, and treatments. Give a patient with pain a $200 budget, say, or directly cover more physical solutions. A prescription in the US often means your treatment is free, but “there ain’t no such thing as a free lunch.” For a percent of genetically predisposed patients, our pharma focus at worst leads to addiction. At best, we’re paying for pain treatments that may not work. In another 2011 Consumer Reports survey of 45,000 patients, pharmaceuticals finished third or fourth in efficacy for non-migraine pain problems. The most effective treatments – massage, physical therapy, ice, chiropractors – are often self-pay. If you’re on disability for pain, are you likely to pay for massage and physical therapy, or get free pills?
CMS sets the standards on safety and efficacy when determining what treatments to cover. Like physicians, they’re highly trained to evaluate pharmaceuticals’ research and polished presentations. Likewise, this approach fails for cost-effective pain relief. Low cost over the counter devices rarely have the funding or resources that pharma has. We pay a lot for drugs because of the high cost of proving efficacy, but since effective devices are rarely reimbursed, there’s no one to bankroll multiple studies and CMS defenses of them. As CEO of a small pain device company, I tried twice to get cold and vibration for pain covered. We had excellent independent data, but at the time we were using the devices for needle pain, which wasn’t a kind of pain CMS wanted to address. We didn’t think about cold and vibration for musculoskeletal pain until much later – and neither did CMS. The result: our devices work great for pennies a use, but are not covered. High intensity TENS units cause muscle vibration, reducing pain. Low intensity units don’t, but the distinction wasn’t noticed at the time. In 2012, CMS stopped paying for ALL of them. Back surgery: covered. Yoga, massage – not so much.
INSURANCE COMPANIES can and should give patients options to pay for data-supported pain treatments before moving to chronic pain meds or surgery. To keep costs down, CMS could allow but cap coverage of FDA-cleared pain devices, massage, or strength classes when data shows they help.
Finally, here’s a story of how a physical approach to pain could reduce pharma use and save money. A smart physical therapist in St. Louis realized that he was seeing a lot of teens with tendinitis a week after coming out of sprained ankle boots. The weak but recovered ankle wasn’t ready to take the strain of full time movement, and got inflamed. The therapist started adding a strong recoiling tape to all his patients once they got out of the boot, and no one got tendinitis any more. The tape corrected the weak motion, providing a physical solution to physical pain. Judicious use of PT resolved his patients’ problems twice as fast as the national average with no medications. Manage movement dysfunction, prevent the pain. At half the cost.
Physical pain has physical solutions. Training away pain is a process, one we need to learn, teach, and pay for. If we can offer alternatives before opioids and take away the power of pain to cause catastrophizing, we can slow the tide of new addictions.